Knock-knees and Bow-legs

Bow-legs
Children with bow-legs (genu varum) stand with their knees not touching, when their ankles are together. Children with knock-knees (genu valgum) stand with their ankles not touching, when their knees are together.
Bow-legs in toddlers are normal. The bowing begins to improve at 18 months of age and continues to improve as the child grows. Bow-legs usually self-correct by the time a child is 3 years old, and the legs typically have a normal appearance. Studies have shown that children with bow-legs walked earlier than average infants (10 months vs 12-15 months). However, if your child has a bow-leg only on one side, or continues to have bow-legs after 3 years old, an x-ray may be needed to make sure your child does not have Blount’s disease. Blount’s disease is a problem of the growth plate in the upper part of the shinbone that causes the bone to be crooked. Bow-legs can also occur due to Rickets. Children with rickets do not get enough calcium, phosphorus, or Vitamin D in their diet—all of which are important for healthy growing bones. Rickets can also occur if a child has a genetic disease that leads to low vitamin D levels.
Knock-knees
Knock-knees are also usually part of the normal growth and development of the legs. Knock-knees are normal in young children and may increase in severity until about age 4. It usually self-corrects by the time a child is 7 or 8 years old. Knock-knees that only appear in a child who is 6 or older, may be a sign of underlying bone disease such as osteomalacia or rickets. Sometimes, an injury to the growth plate of the shinbone or tumours may cause either knock-knees or bow-legs.
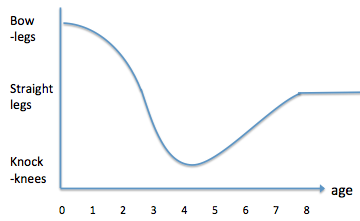 Normal development of leg alignment
Normal development of leg alignment
When does bow-legs or knock-knees require an orthopaedic referral?
Not all bow-legs or knock-knees need an orthopaedic referral. See a doctor if your child’s bow-legs or knock-knees is only on one-side, falls outside the age range of normal leg development, is substantially deformed or progressively getting worse, is associated with poor balance or pain, or if there are limitations in activities.
Treatment
Most young children with bow-legs or knock-knees grow out of it without needing any special splints or shoes. However, if your child has low muscle tone, it will be useful for a paediatric physiotherapist to assess your child’s feet, leg alignment and hip rotation range of movement. The position of your child’s feet and hips will affect the posture of the knees. A child with knock-knees may also have feet and hips that roll inwards, whereas a child with bow-legs is more likely to have feet and hips that roll outwards. In such situations, special splints that support your child’s feet in good alignment, or strengthening of specific weak muscles will be helpful.
Don’t force your child to stand and walk when he is not ready. Ensure that he has sufficient muscle strength to maintain good leg alignment. The fear of falling during forced standing or walking will cause your child to adopt postures that place stresses on the wrong parts of the body, leading to long-term musculoskeletal disorders. Poor alignment of the legs during forced standing and walking places un-natural pressure either on the outside or inside of the knee joints, contributing to bow-legs or knock-knees.
Blount’s disease:
Toddlers with Blount’s disease may need to be treated with braces. If the brace does not correct the bowing, surgery is usually recommended by the age of 4. Teenagers with Blount’s disease need surgery to correct the bowing.
Rickets:
If the Rickets is properly treated with medication, the bowing may correct on its own. Surgery is needed if the bowing does not improve after medication.
Outcomes
Toddlers with typical bow-legs or knock-knees develop normally and do not have any long-term problems. Older children and teenagers may not have spontaneous improvement in their alignment. If they have significant pain, limitations of activities, or substantial deformity, surgery may be required.
Toddlers with Blount’s disease do very well if they are diagnosed and treated early. Overweight patients with adolescent Blount’s disease have a higher risk of the bowed legs recurring after treatment.
Please feel free to reach out to us if your kid needs an assessment to determine if treatment is needed.
Let's get in touch