Clubfoot (CTEV)
 Normal L foot L Clubfoot
Normal L foot L Clubfoot
Introduction
Clubfoot is a congenital deformity of the foot, and is also known as ‘Congenital Talipes EquinoVarus’ (CTEV). It is one of the most common congenital abnormalities to affect the foot. It is caused by an abnormal development of a baby’s bones, ligaments and muscles of his foot while he is in the womb. If not treated, clubfoot can make it difficult and painful to walk, affecting a person’s mobility. Clubfoot presents as malalignment of the foot structures in the hindfoot, midfoot and forefoot. It affects the structure and position of the foot, resulting in an inward turning of the midfoot and a varus hindfoot. The foot is held in a fixed downward pointing position. The foot affected by clubfoot tends to be shorter. Clubfoot can be either positional or structural. Positional clubfoot is when the foot is able to actively correct its posture when stimulated. Structural clubfoot is not passively correctable and presents with varying degrees of stiffness.
Treatment
The goal of clubfoot treatment is to provide long-term correction of the deformity, resulting in a foot that is fully functional and pain-free. Clubfoot treatment is divided into two main approaches: Conservative or Surgical. Conservative treatments (which include the Ponseti method and the French method) correct clubfoot by slowly stretching tight structures, allowing time for soft tissue remodelling. Surgical treatment of clubfoot lengthens bony or soft tissue structures that are tight or deformed.
Ponseti's Method

The Ponseti Method was developed by Dr Ponseti, an Orthopaedic Surgeon, after extensive anatomical study of the foot. It has been shown to be safer and more efficient than surgery for the treatment of clubfoot. When done correctly, results of the Ponseti Method can achieve full correction of the clubfoot deformity in up to 98% of cases. Long-term follow-up showed excellent treatment results in foot function.
Steps of Ponseti’s method:
1. Weekly Stretching and Casting of foot for about 6-8 weeks
The Ponseti technique uses a very specific series of stretches and castings to correct the foot deformity. The casting is a set of casts that slowly bring the foot around to a neutral position. Each week, the baby’s foot is gently manipulated and a cast is placed from the toes to the upper thigh. With each week’s cast, the position improves. This usually takes about 6 to 8 weeks.
2. Achilles Tenotomy: cut through Achilles Tendon
At the end of the 6-8 weeks, the orthopaedic doctor does a very small incision to lengthen the tight Achilles tendon. This eliminates the equinus deformity. This is followed by a further three weeks in a cast. Once this last cast comes off, the foot should be in a neutral, corrected position.
3. Bracing (Foot Abduction Brace) to maintain the correction:
If left alone at this point, there is a high chance of relapse, so the baby must wear a foot abduction brace (boots set apart and turned outwards, on a bar). This brace maintains the correction. The baby must wear the brace full-time for 2-3 months and then nightly for the next few years.

 Examples of boots with the Denis Browne bar
Examples of boots with the Denis Browne bar
It is very important for parents to make sure the baby wears the brace. The most common reason for the clubfoot position to recur is not wearing the brace. If the clubfoot position does recur, the baby will need to be casted again. The baby might need to have the Achilles tendon lengthened again or additional surgery.
The French Method
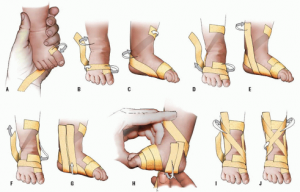 (From Noonan KJ, Richards BS. Nonsurgical management of idiopathic clubfoot. J Am Acad Orthop Surg 2003;11:392-402)
(From Noonan KJ, Richards BS. Nonsurgical management of idiopathic clubfoot. J Am Acad Orthop Surg 2003;11:392-402)
The French Method consists of daily stretches of the baby's clubfoot, and stimulation of the muscles acting on the foot to maintain the range of movement achieved through the stretches. The foot is then taped using nonelastic adhesive strapping. It takes longer to get a normal foot position with stretching. Treatment usually lasts over a course of approximately two months and is then gradually reduced. The parents are taught to do the stretches at home too. The baby may still need to have the Achilles tendon lengthened. These babies wear splints until age 2 or 3.
When the Ponseti and French methods were compared, the Ponseti method showed a slightly better clinical outcome. This may be due to the amount of effort required to train the parents and have them implement the technique reliably (i.e. perform the stretching, taping, and splinting on a daily basis) for up to two years.
Surgery
In bad cases of clubfoot, surgery may be needed to correct the foot position. This can involve lengthening or transferring tendons. Metal pins can be used to hold the bones in their new position. The foot will be put in a cast after surgery. Studies have found high levels of foot and ankle stiffness and weakness amongst patients ten years after surgery. This and other evidence led to the current opinion by most orthopaedic clinicians: that clubfoot should ideally be managed conservatively.
Please feel free to reach out to us if you have any questions.
Let's get in touch